
By: Cheryl Rice, DVM, DACVIM, GDVWHM, CHPV
Published: July 16, 2026
At the current time, our previous assay for PTHrP (parathyroid hormone-related protein) remains unavailable. We understand this affects our clients’ daily practice and wish to extend our appreciation for your ongoing patience as we actively work toward a new testing method. During this time, the following assays are encouraged:
- Basic Parathyroid Panel | Test Code 20033 | Includes: PTH, iCa
- Vitamin D Panel | Test Code 20035 | Includes: PTH, iCa, 25-hydroxyvitamin D
Quick PTHrP Refresher
Parathyroid hormone-related protein (PTHrP) is a small peptide protein that shares structural similarities to parathyroid hormone (PTH). PTH is produced solely in the parathyroid glands and is released into systemic circulation to regulate calcium homeostasis. PTHrP is produced by a wide variety of cells, but its actions are normally restricted to local influence on adjacent tissues. Neoplastic transformation of these cells can lead to over-expression of PTHrP with systemic distribution and binding to targets normally intended for PTH, resulting in humoral hypercalcemia of malignancy (HHM). While a positive PTHrP result provides support for the presence of humoral hypercalcemia of malignancy, a negative PTHrP result does not eliminate the possibility of malignancy as there are multiple other mechanisms by which cancers can cause hypercalcemia. (Feldman and Nelson, Astanopoulou, Schluter, Cheloha, Wei MIng Chang, Bolliger).
Summary:
- A positive PTHrP result provides support for a diagnosis of hypercalcemia of malignancy.
- PTHrP is the most common (but not the only) marker of HHM, and HHM can exist in the presence of a negative PTHrP.
- Infrequently, false positive PTHrP results (e.g., a persistent positive result in the absence of any detectable abnormality in the patient over time) can exist, which is most often noted in cats.
- Lastly, positive PTHrP results may co-exist in the presence of ectopic PTH elevation.
Commonly Encountered Patterns of Results and Their Interpretations
Under normal physiologic conditions, calcium is tightly regulated. It may be helpful to think of PTH as a thermostat sensing the environment and directing the actions of the furnace, and iCa the temperature of the room. In this analogy, setting the thermostat higher (PTH) is expected to increase the temperature (iCa) in a room by sending a message to the furnace to liberate more heat, and vice versa. When the thermostat senses the appropriate temperature is reached, it ceases to send a signal. Similarly, when the parathyroid gland senses an appropriate level of ionized calcium is reached, it ceases to send a signal to liberate calcium from other sources in the body. This is the process of normal negative feedback.
Both in this analogy and in physiology, however, there is some lag time between the request and the response, so some gray areas are unavoidable, as the body must either mobilize or de-mobilize calcium in the blood stream. In other words, endocrinology exists in perpetual motion in the body, and when we observe it as a single point in time, our perspective may at times be incomplete.
Normal Calcium Homeostasis: Normal PTH with Normal iCa
When the set temperature of the thermostat and the temperature of the room are the same (or appropriate to one another in terms of their reference intervals), this suggests normal or functional environmental controls. This is akin to PTH and ionized calcium concentrations within their normal reference intervals and reflect normal calcium homeostasis. Under these conditions, even if there is suspicion of neoplasia based on other clinical signs, there is no additional benefit in a PTHrP assay, as hypercalcemia is not present.
Example 1:
A 6-year-old male neutered Domestic Shorthair presented for evaluation of polyuria/polydipsia.
-
PTH0.70-3.40 pmol/L1.25 pmol/L
-
iCa1.00-1.40 mmol/L1.31 mmol/L
-
25-hydroxyvitamin D93-327 nmol/L112 nmol/L
Interpretation:
Concentrations of ionized calcium and parathyroid hormone are within their respective reference intervals. These results reflect adequate calcium homeostasis currently. The concentration of 25-hydroxyvitamin D is within the reference interval, suggesting adequate intake and absorption of vitamin D.
Primary Hyperparathyroidism (Parathyroid Dependent Hypercalcemia): High PTH and High iCa
What about when the thermostat is set at a particular temperature, but the environmental temperature exceeds this? In primary hyperparathyroidism, one or more parathyroid glands (the furnace) continue to produce PTH without regard for negative feedback from the thermostat and overriding the request to cease liberating calcium (heat). Because the misbehavior arises from the parathyroid glands themselves, this is termed primary hyperparathyroidism. In most cases, there is no additional benefit in a PTHrP result in this scenario, as an increased concentration of PTH provides an explanation for increased ionized calcium.
If the ionized hypercalcemia had been the result of an increased concentration of PTHrP, then negative feedback mechanisms would normally serve to suppress PTH at least into the lower third of the reference interval. There are very rare cases, however, wherein primary hyperparathyroidism could coexist with humoral hypercalcemia of malignancy. In these unusual circumstances, both PTH and PTHrP could be inappropriately increased.
Example:
13-year-old female spayed Shih Tzu has elevated total calcium noted on routine annual lab screening. May be drinking/urinating more, although the change has been very gradual and the owner wonders whether it may just be a reflection of the warmer weather.
-
-
PTH1.10-10.60 pmol/L13.0 pmol/L↑
-
iCa1.25 – 1.45 mmol/L1.57 mmol/L↑
-
25-hydroxyvitamin D112-366 nmol/L172 nmol/LN
Interpretation:
This concentration of parathyroid hormone is inappropriately increased in association with hypercalcemia. The results of this profile are consistent with a diagnosis of primary hyperparathyroidism. The 25-hydroxyvitamin D concentration is within the reference interval and not suggestive of excessive dietary intake of vitamin D as the cause of hypercalcemia.
Secondary Hyperparathyroidism: High PTH with normal to low iCa
What about when the thermostat setting is higher than the actual room temperature? In physiologic terms, we could interpret that a proper request is being given, but there is an inability to elicit the proper response from the body. This lack of response could result from inadequate intake, absorption, or metabolism of dietary calcium and/or vitamin D (25-hydroxyvitamin D and/or calcitriol) to provide the proper response, or it could occur due to excessive loss of calcium or 25-hydroxyvitamin D from the gastrointestinal or urinary tract or as a result of compensating for other abnormalities in the body.
In the first scenario (inadequate intake/absorption), we would consider differentials of unbalanced diet, significant gastrointestinal disease, genetic conditions such as rickets, and/or underlying renal disease. In the second scenario, loss of calcium and 25-hydroxyvitamin D could occur through the gastrointestinal or urinary tract (protein-losing enteropathy, protein-losing nephropathy), or as a result of other endocrinopathies, such as canine hyperadrenocorticism or feline hyperthyroidism.
Because the problem lies somewhere in the body other than the parathyroid glands (i.e., the problem is in the response and not in the request), this is termed secondary hyperparathyroidism. Because ionized hypercalcemia is by definition not present in secondary hyperparathyroidism, a PTHrP assay adds no additional benefit given this pattern of results.
Example 1:
A 14-year-old male neutered Domestic Shorthair cat has a history of progressive renal disease (currently IRIS stage 3).
-
-
PTH0.70-3.40 pmol/L7.50 pmol/L↑
-
iCa1.00-1.40 mmol/L1.19 mmol/LN
-
25-hydroxyvitamin D93-327 nmol/L134 nmol/LN
-
Calcitriol13-145 pmol/L<12.5 pmol/L↓
Interpretation:
These results (increased concentration of parathyroid hormone in combination with normocalcemia) reflect a status of secondary hyperparathyroidism, which is typically due to chronic renal disease, a nutritional deficiency of vitamin D, or both. The 25-hydroxyvitamin D concentration is within the reference interval, decreasing the likelihood of insufficient dietary intake and absorption of vitamin D as a cause. The concentration of calcitriol is decreased, suggesting that renal disease is the likely cause of secondary hyperparathyroidism in this case.
Example 2:
A 9-year-old spayed female Yorkshire Terrier has a history of protein-losing enteropathy and clinical signs of poor appetite, intermittent diarrhea and weight loss.
-
-
PTH1.10-10.60 pmol/L18.5 pmol/L↑
-
iCa1.25-1.45 mmol/L1.17 mmol/L↓
-
25-hydroxyvitamin D112-366 nmol/L39 nmol/L↓
Interpretation:
These results (increased concentration of parathyroid hormone in combination with mild hypocalcemia) reflect a status of secondary hyperparathyroidism, which is typically due to chronic renal disease, nutritional deficiency of vitamin D, or both. This significantly decreased concentration of 25-hydroxyvitamin D suggests inadequate dietary intake and/or intestinal malabsorption of vitamin D is a likely cause, or at least contributory. Chronic gastrointestinal disease may be a cause of vitamin D and/or calcium malabsorption. Urinary loss of vitamin D metabolites has also been described in association with proteinuric renal disease.
Parathyroid Independent Hypercalcemia : Low Normal to Low PTH concentration with increased ionized calcium concentration.
When calcium is increased in the absence of an increased PTH concentration, then we know that there is another cause for the hypercalcemia. That is, the problem has developed independently from the parathyroid gland. Using the thermostat analogy, this is described by a situation where the thermostat and furnace have been turned down very low, or off, but the room remains much too hot. The conclusion is that there is another source of heat. Is it a warm day, is something cooking in the oven, or is the house on fire? Further investigation is warranted.
The most common causes of parathyroid independent ionized hypercalcemia in dogs are humoral hypercalcemia of malignancy and hypoadrenocorticism. Other possible causes in dogs include excess ingestion of 25-hydroxyvitamin D (through supplements or rodenticide), exposure/ingestion of topical anti-psoriasis creams (which contain calcipotriene), and granulomatous disease (which may be seen with fungal disease, chronic skin inflammation or Schistosomiasis in dogs).
In cats, common causes include humoral hypercalcemia of malignancy and idiopathic hypercalcemia. Oral 25-hydroxyvitamin D excess is also seen in cats, whether the result of feed mis-formulation or ingestion of supplements. Hypercalcemia due to hypoadrenocorticism, acute and chronic renal disease, elevated dietary Ca:P ratio and calcium containing phosphate binders are seen in cats. Mild ionized hypercalcemia has been noted sporadically with SGLT2 inhibitor therapy, and with lactulose therapy.
Parathyroid-independent ionized hypercalcemia represents a pattern of results where concurrent measurement PTHrP may be beneficial, and our efforts to restore this assay remain active.
Example 1:
A 6-month-old Saint Bernard puppy was running off-lead and was observed eating something on the ground, but the owner could not determine what it had been. Three days later, he is very lethargic, polyuric/polydipsic, vomiting and his renal values are increased.
-
-
PTH1.10-10.60 pmol/L<0.5 pmol/L↓
-
iCa1.25-1.45 mmol/L1.86 mmol/L↑
-
25-hydroxyvitamin D112-366 nmol/L>1800↑
Interpretation:
The low concentration of parathyroid hormone reflects appropriate suppression in association with clinically significant ionized hypercalcemia. This 25-hydroxyvitamin D concentration is markedly increased, indicating that the hypercalcemia is due to hypervitaminosis D. This is most consistent with recent exposure to vitamin D containing compounds, including rodenticide.
Example 2:
A 12-year-old spayed female Golden Retriever presented for evaluation of progressive weight loss, lethargy and polyuria/polydipsia. Physical exam revealed prominent enlarged peripheral lymph nodes.
-
-
PTH1.10-10.60 pmol/L<0.5 pmol/L↓
-
iCa1.25-1.45 mmol/L1.65 mmol/L↑
-
25-hydroxyvitamin D112-366 nmol/L221 nmol/LN
Interpretation:
The low concentration of parathyroid hormone is indicative of parathyroid independent hypercalcemia. The most common differential diagnosis given this pattern of results is hypercalcemia of malignancy. Granulomatous disease may be an additional differential diagnosis, particularly if there is concurrent hyperphosphatemia. Hypoadrenocorticism is also a differential diagnosis for parathyroid independent hypercalcemia. If there are clinical signs which increase suspicion and this dog has not received any exogenous steroids recently, then measurement of baseline cortisol could rule out such a diagnosis. The 25-hydroxyvitamin D concentration is within the reference interval and not suggestive of excessive intake of vitamin D as the cause of hypercalcemia.
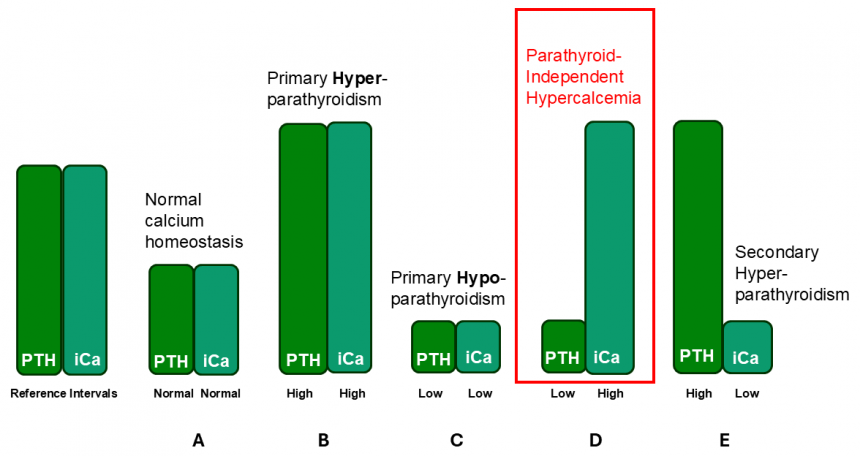
Figure 1: Patterns of PTH and ionized Calcium
References
Anastasopoulou C, Mewawalla P. Malignancy-Related Hypercalcemia. 2025 Mar 4. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan–. PMID: 29494030.
Bolliger, A.P., Graham, P.A., Richard, V., Rosol, T.J., Nachreiner, R.F. and Refsal, K.R. (2002), Detection of Parathyroid Hormone—Related Protein in Cats with Humoral Hypercalcemia of Malignancy. Veterinary Clinical Pathology, 31: 3-8. https://doi.org/10.1111/j.1939-165X.2002.tb00268.x
Cheloha RW, Gellman SH, Vilardaga JP, Gardella TJ. PTH receptor-1 signalling-mechanistic insights and therapeutic prospects. Nat Rev Endocrinol. 2015 Dec;11(12):712-24. doi: 10.1038/nrendo.2015.139. Epub 2015 Aug 25. PMID: 26303600; PMCID: PMC4651712.
Feldman and Nelson Textbook
Kohart NA, Elshafae SM, Breitbach JT, Rosol TJ. Animal Models of Cancer-Associated Hypercalcemia. Vet Sci. 2017 Apr 13;4(2):21. doi: 10.3390/vetsci4020021. PMID: 29056680; PMCID: PMC5606604.
Parathyroid Hormone-Like Hormone is a Poor Prognosis Marker of Head and Neck Cancer and Promotes Cell Growth via RUNX2 Regulation
Wei-Min Chang, Yuan-Feng Lin, Chia-Yi Su, Hsuan-Yu Peng, Yu-Chan Chang, Jenn-Ren Hsiao, Chi-Long Chen, Jang-Yang Chang, Yi-Shing Shieh, Michael Hsiao, Shine-Gwo Shiah DOI: 10.1038/srep41131